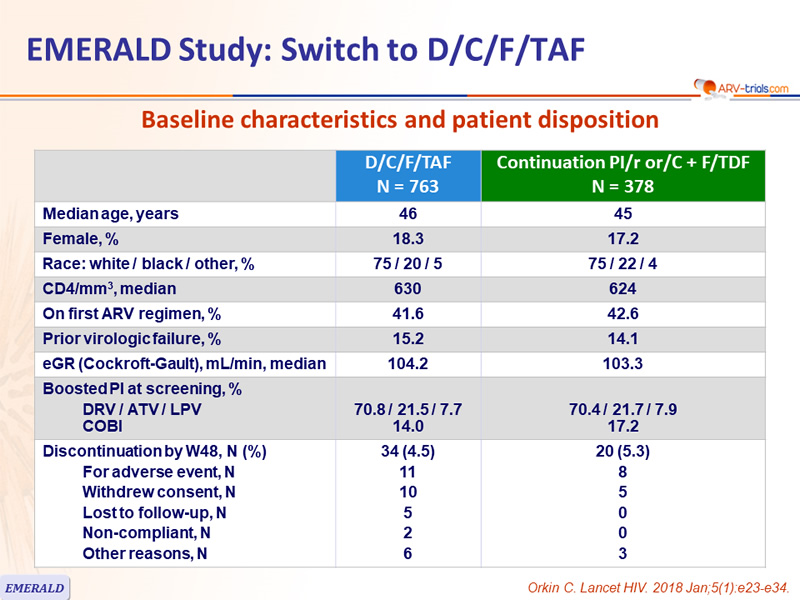
Baseline characteristics and patient disposition
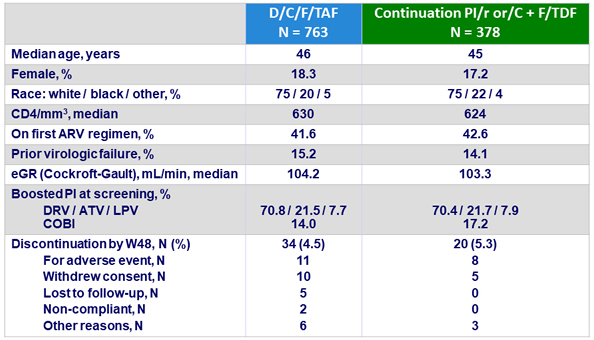
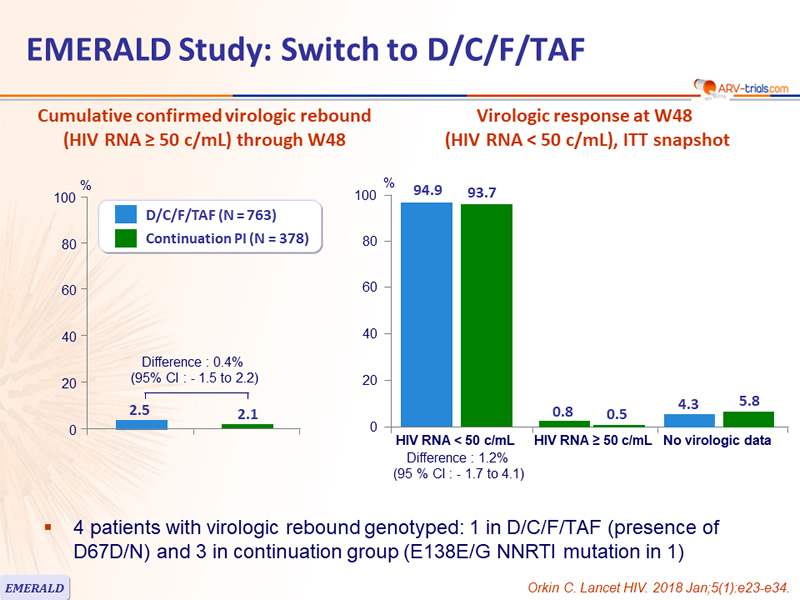
- 4 patients with virologic rebound genotyped: 1 in D/C/F/TAF (presence of D67D/N) and 3 in continuation group (E138E/G NNRTI mutation in 1)
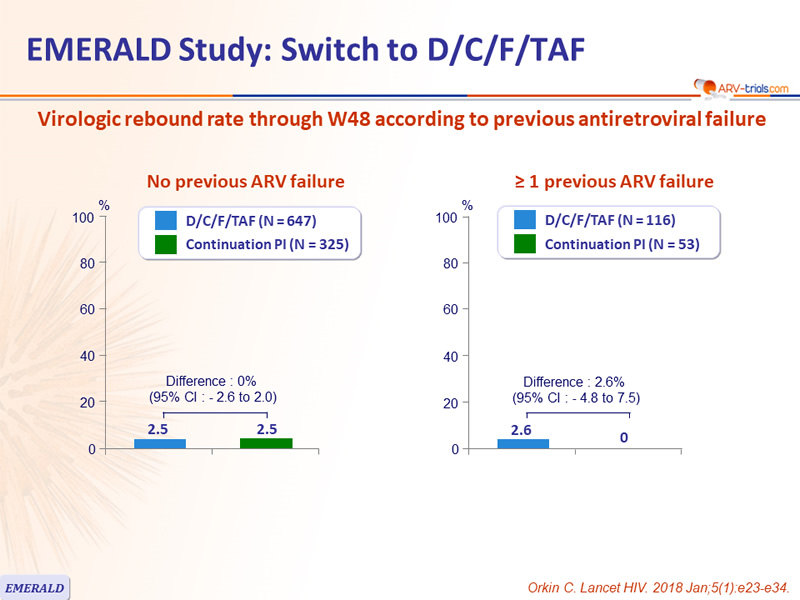
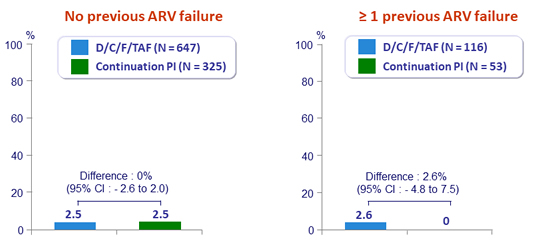
Virologic rebound rate through W48 according to previous antiretroviral failure
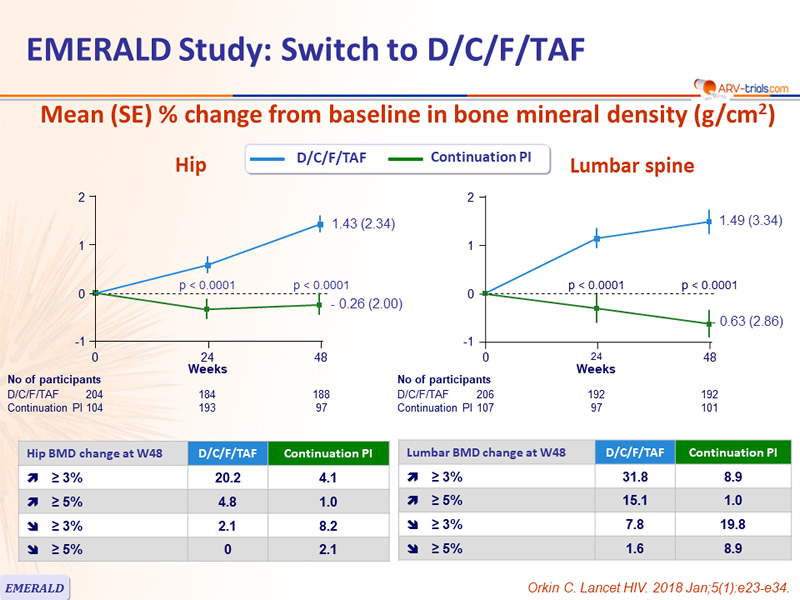
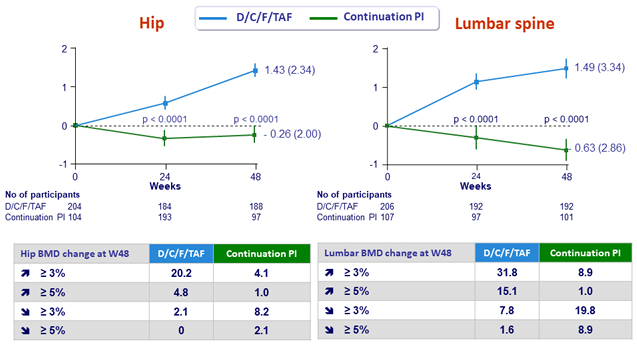
Mean (SE) % change from baseline in bone mineral density (g/cm²)
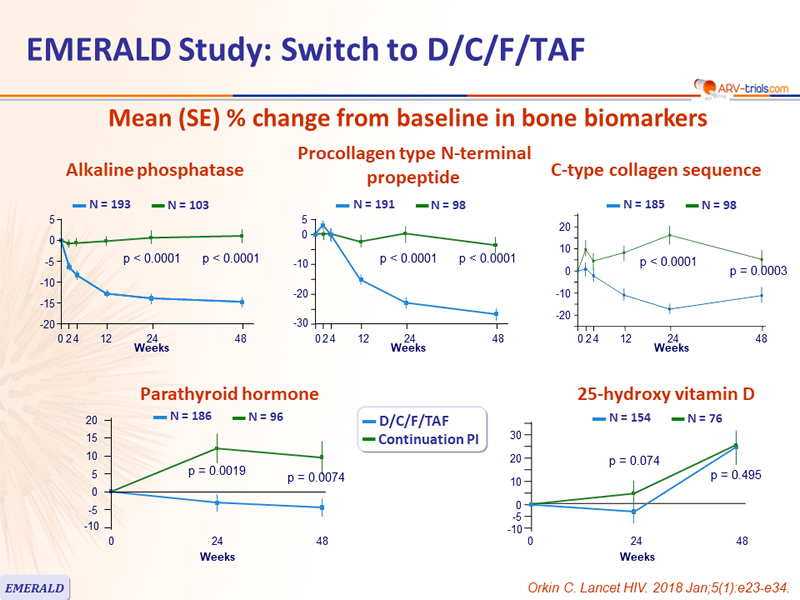
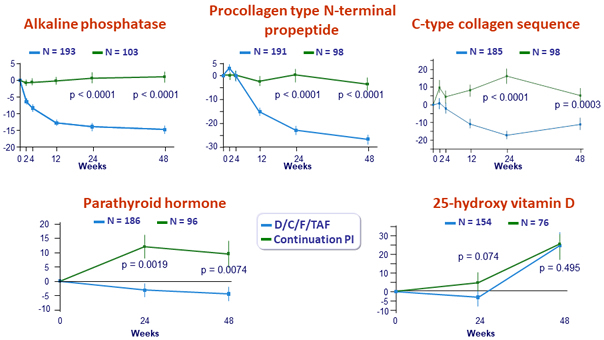
Mean (SE) % change from baseline in bone biomarkers
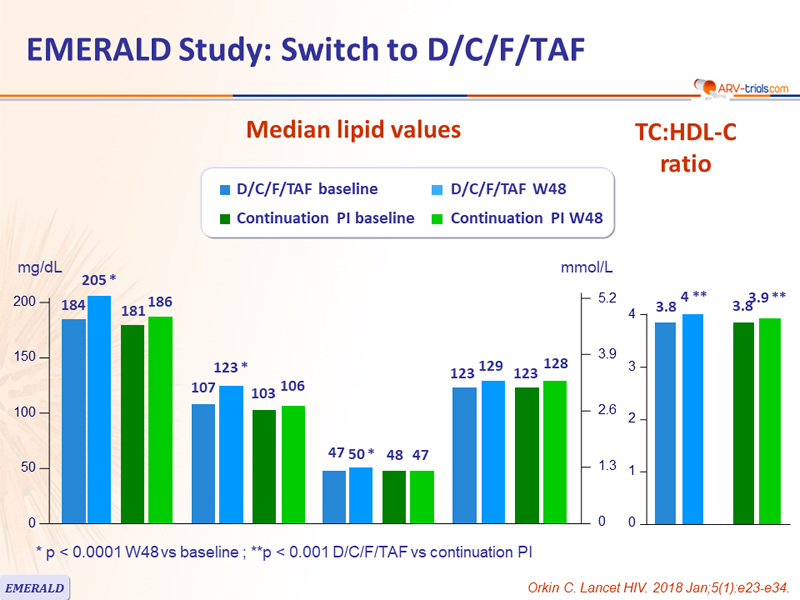
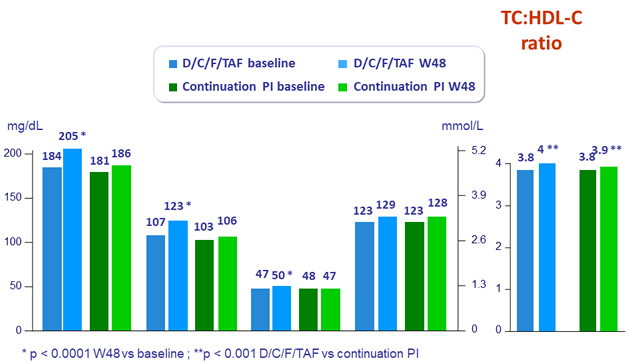
Median lipid values
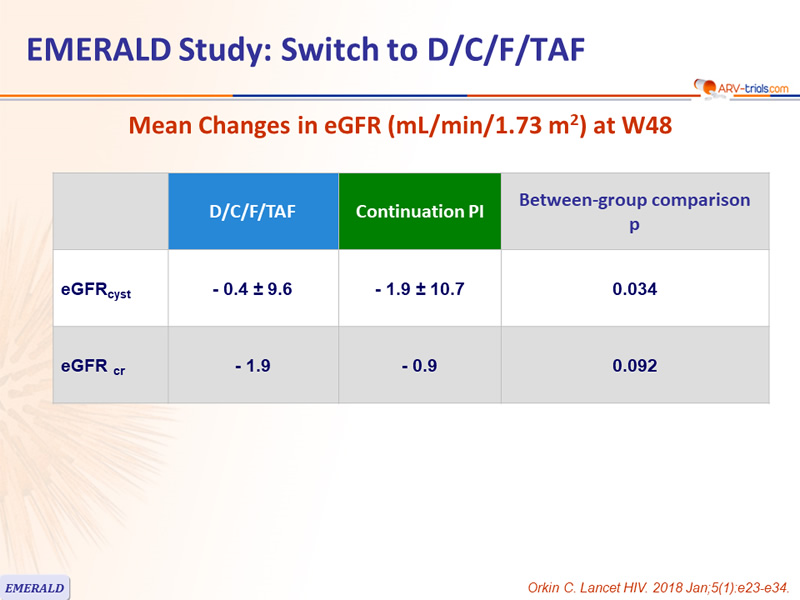
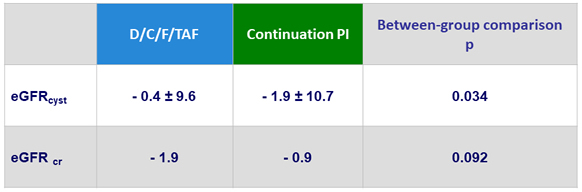
Mean Changes in eGFR (mL/min/1.73 m²) at W48
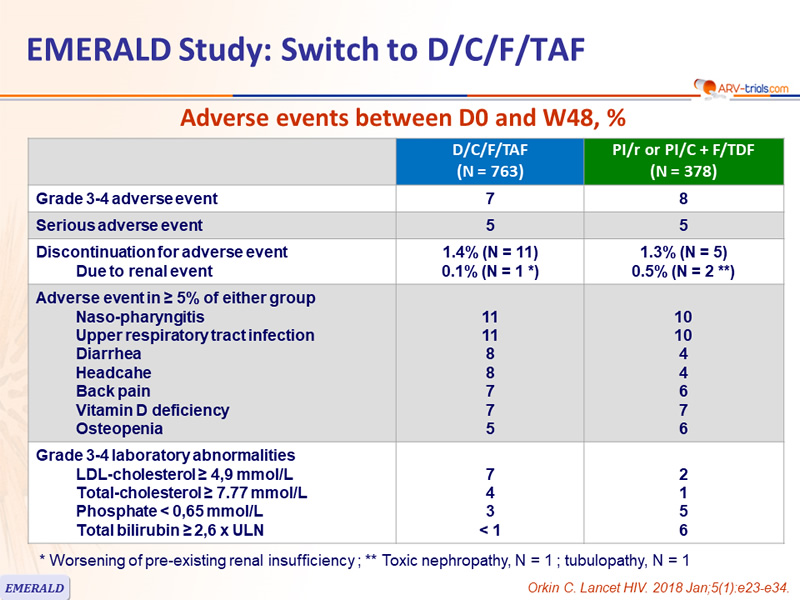
Adverse events between D0 and W48, %
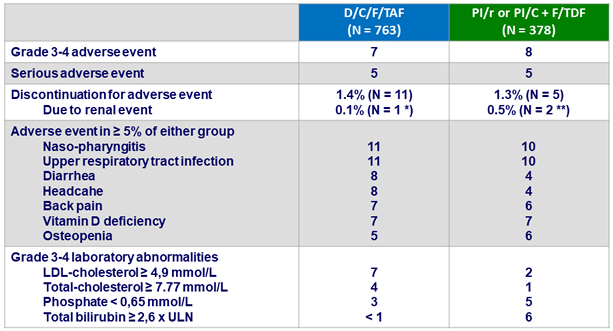
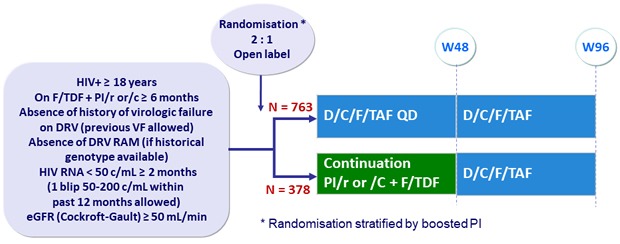
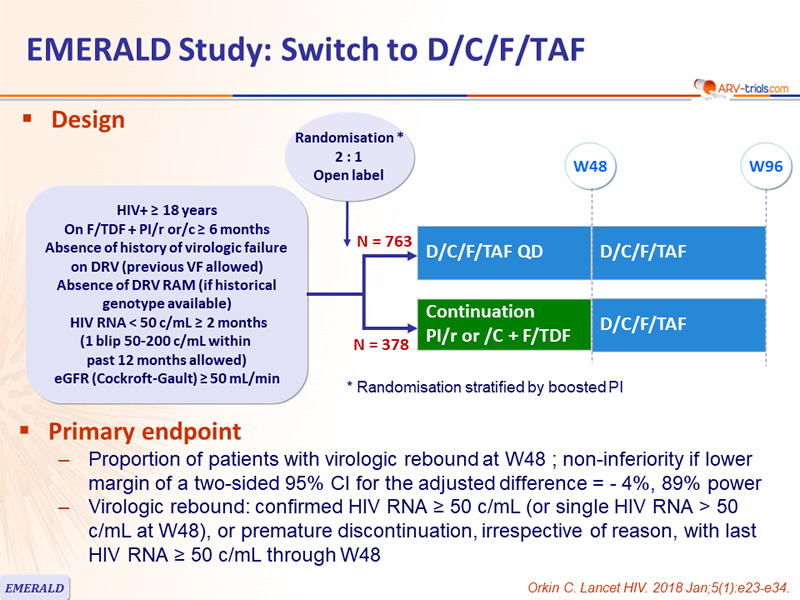
*
Worsening of pre-existing renal insufficiency ; ** Toxic nephropathy, N = 1 ; tubulopathy , N = 1