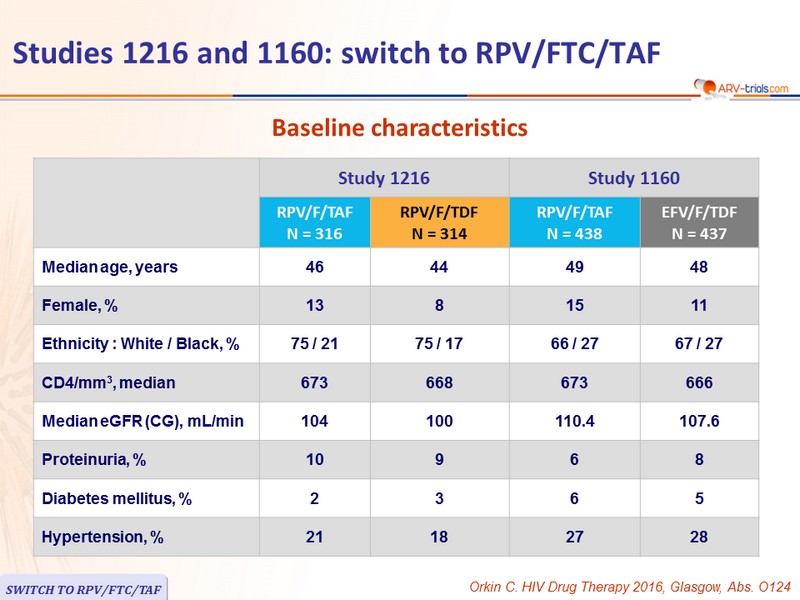
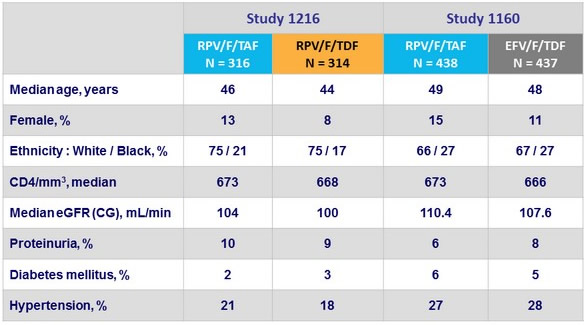
Baseline characteristics
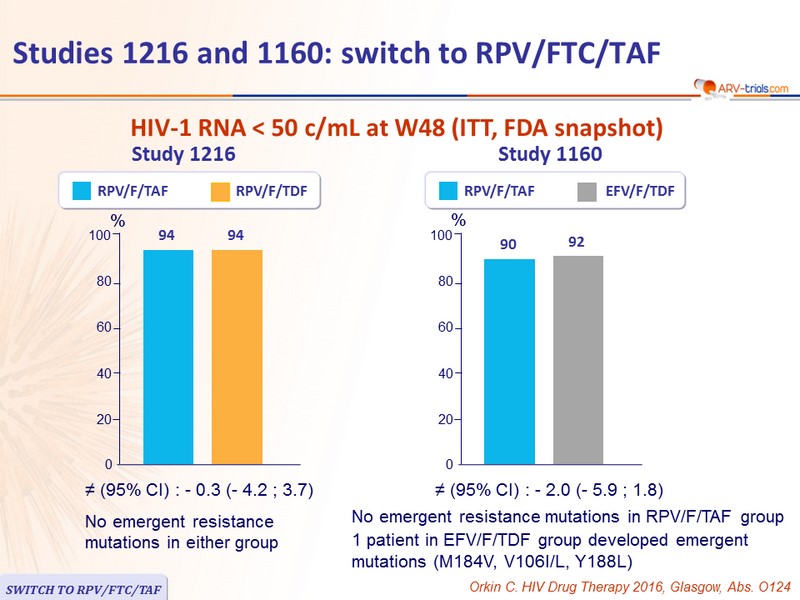
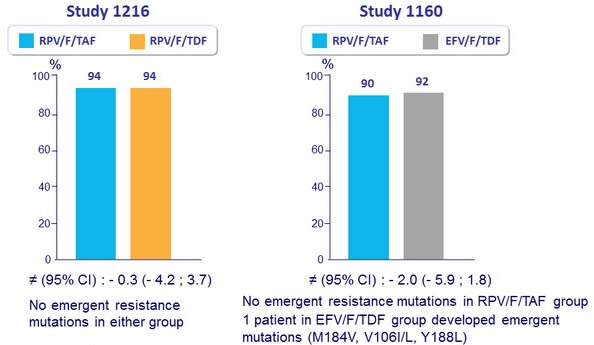
HIV-1 RNA < 50 c/mL at W48 (ITT, FDA snapshot)
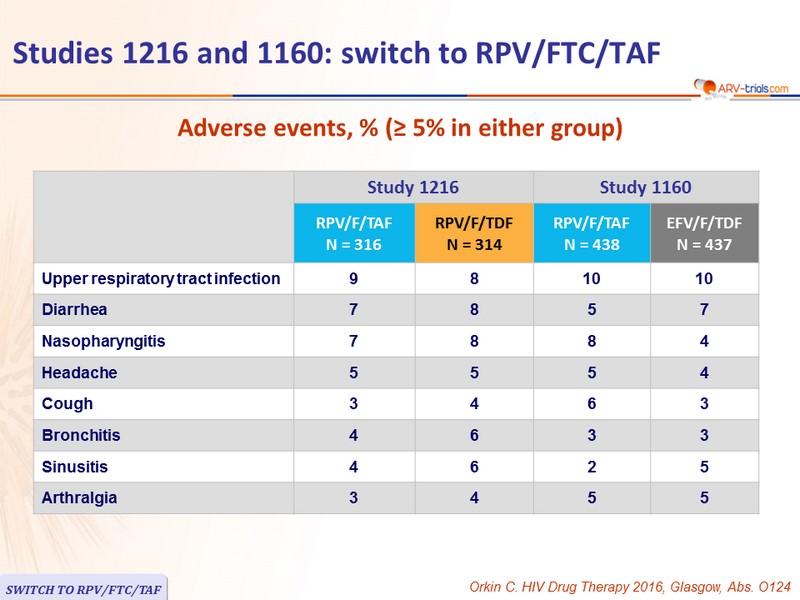
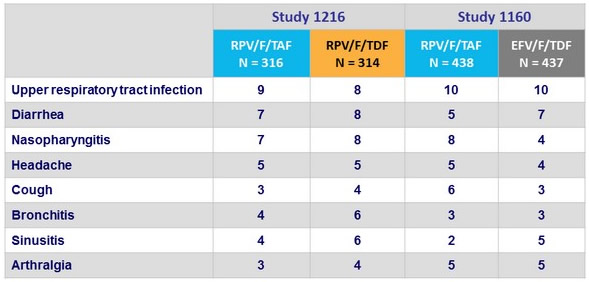
Adverse events, % (≥ 5% in either group)
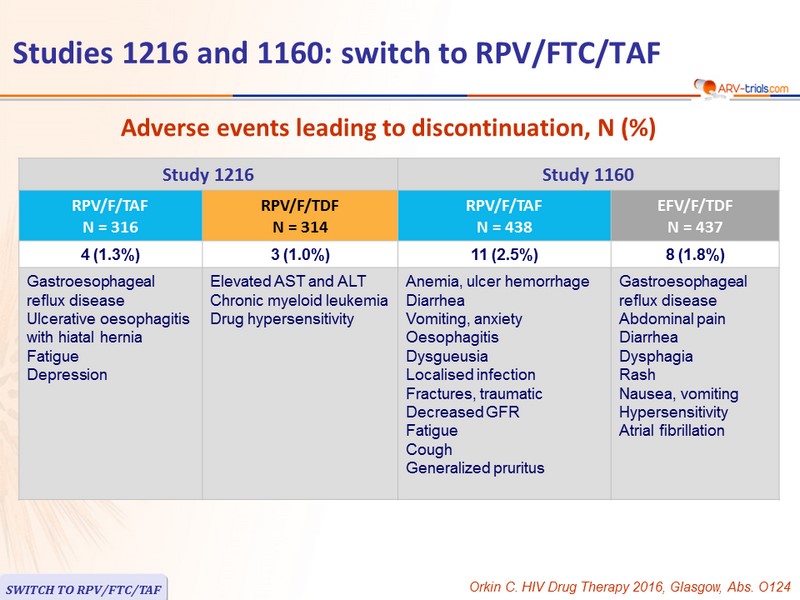
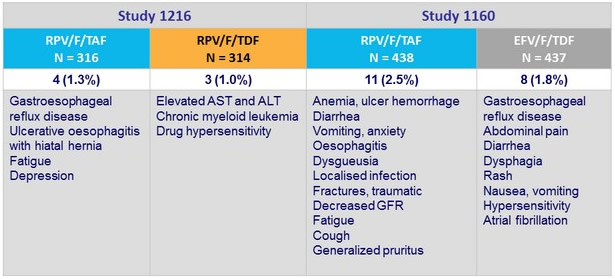
Adverse events leading to discontinuation, N (%)
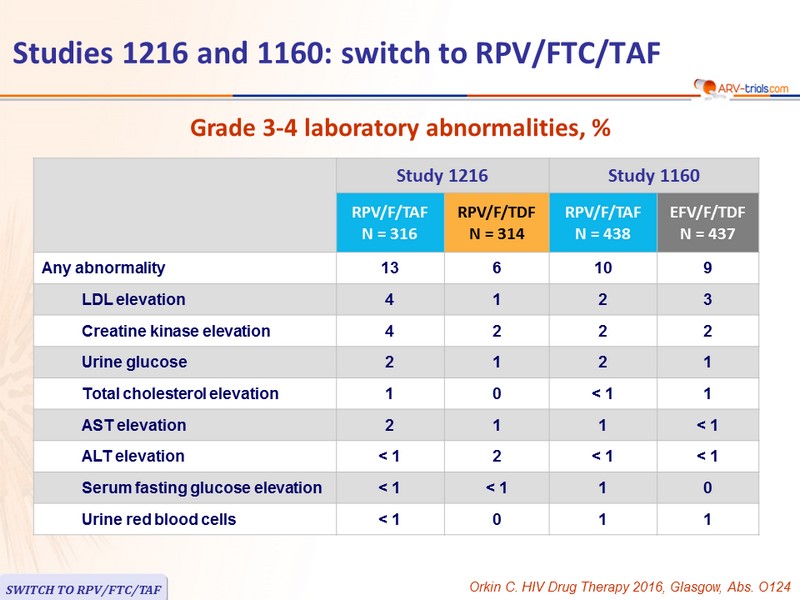
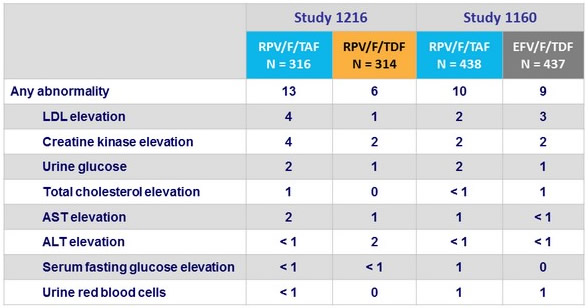
Grade 3-4 laboratory abnormalities, %
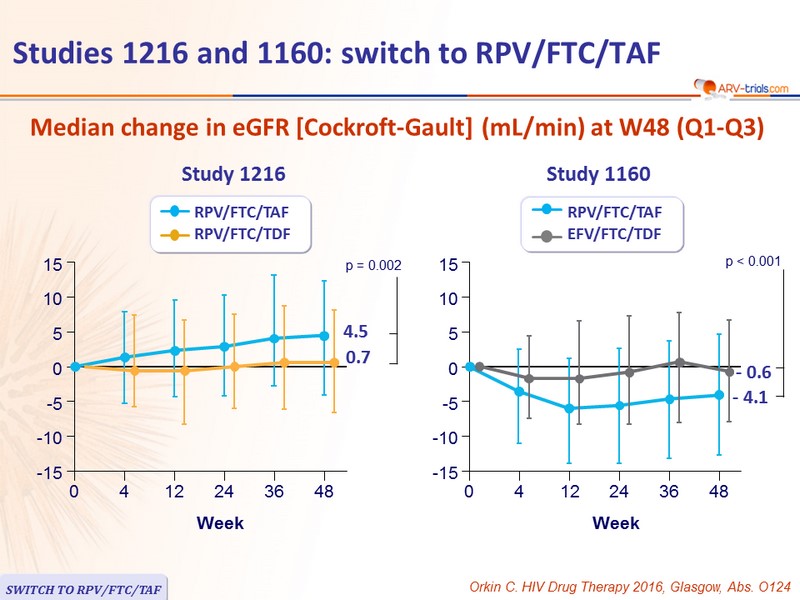
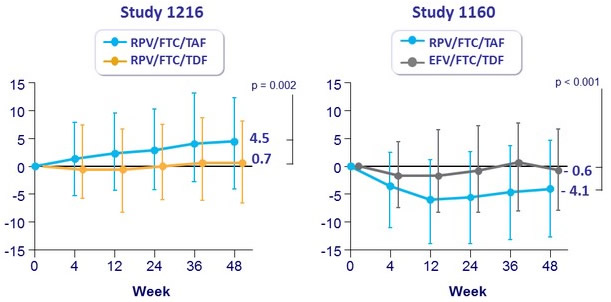
Median change in eGFR [ Cockroft-Gault ] (mL/min) at W48 (Q1-Q3)
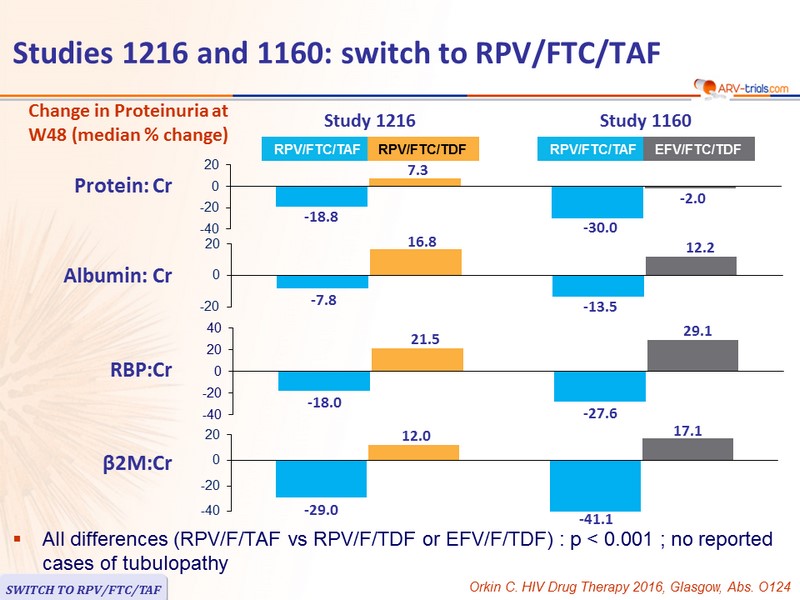
Change in Proteinuria at W48 (median % change)
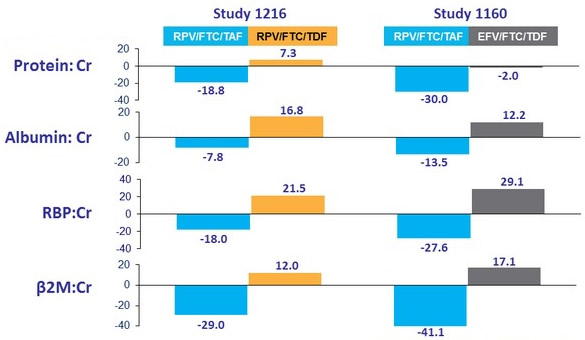
- All differences (RPV/F/TAF vs RPV/F/TDF or EFV/F/TDF) : p < 0.001 ; no reported cases of tubulopathy
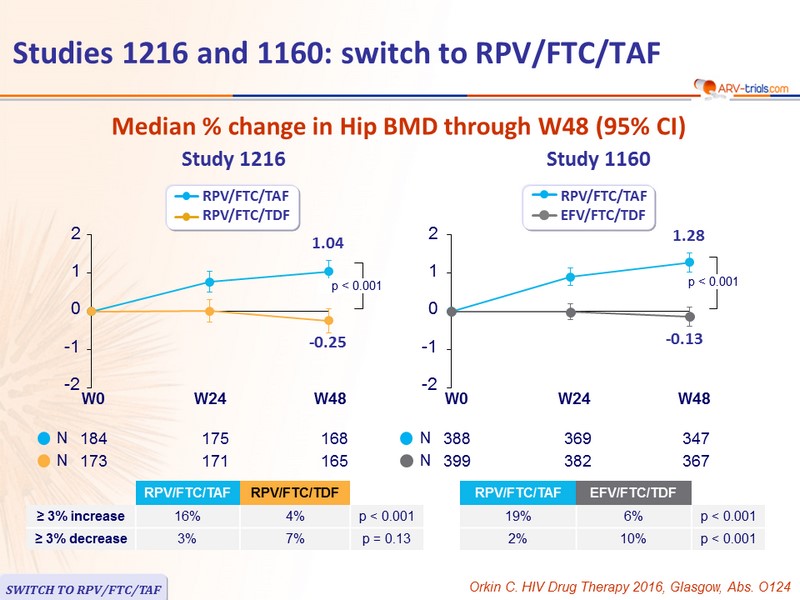
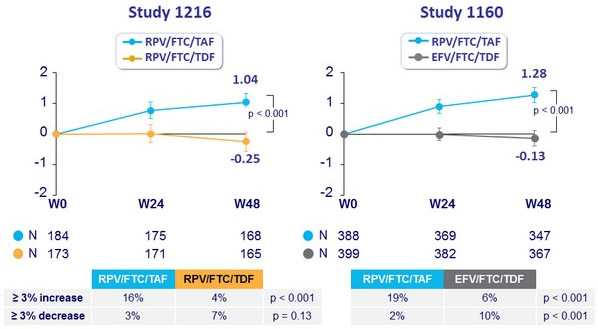
Median % change in Hip BMD through W48 (95% CI)
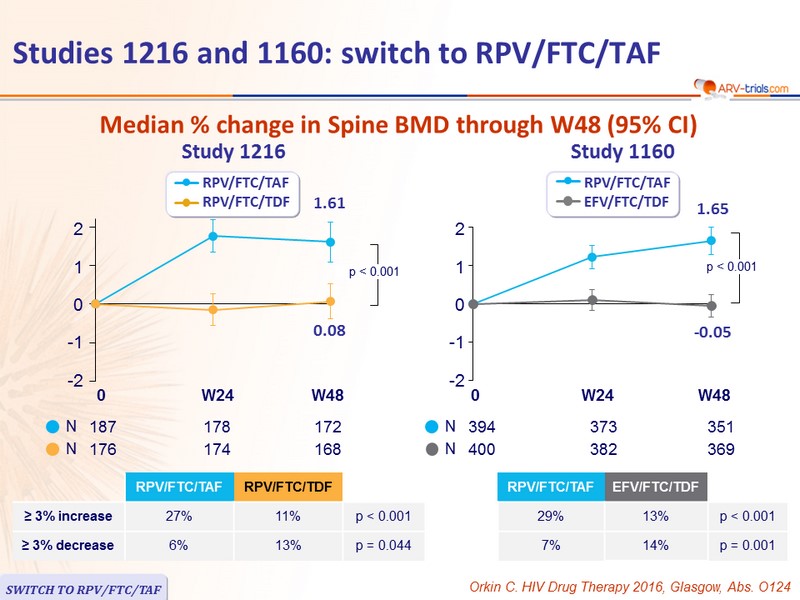
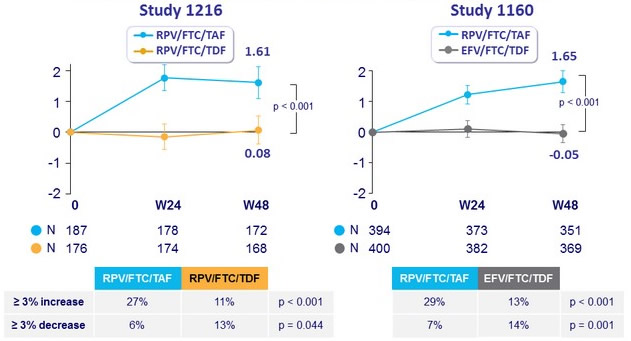
Median % change in Spine BMD through W48 (95% CI)
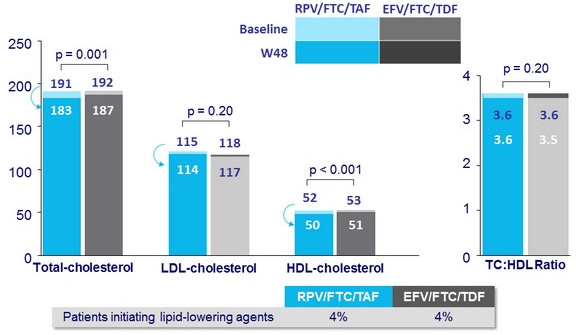
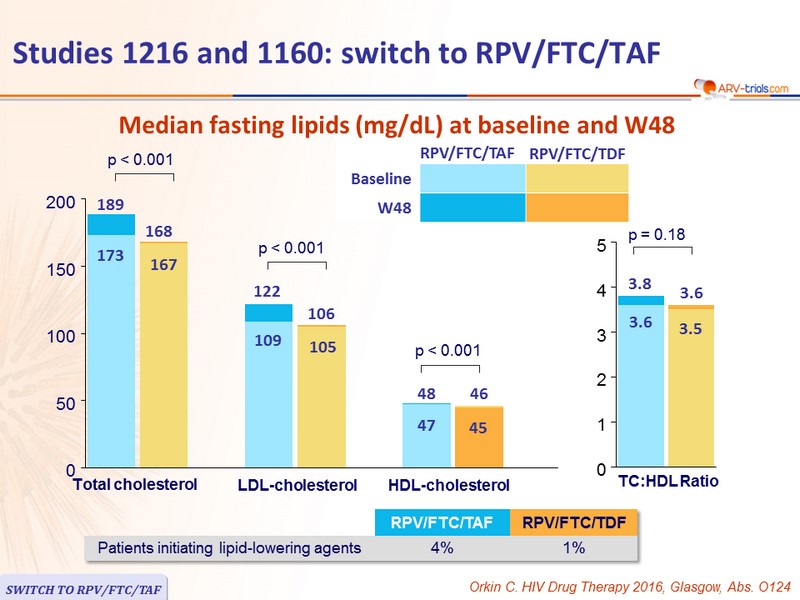
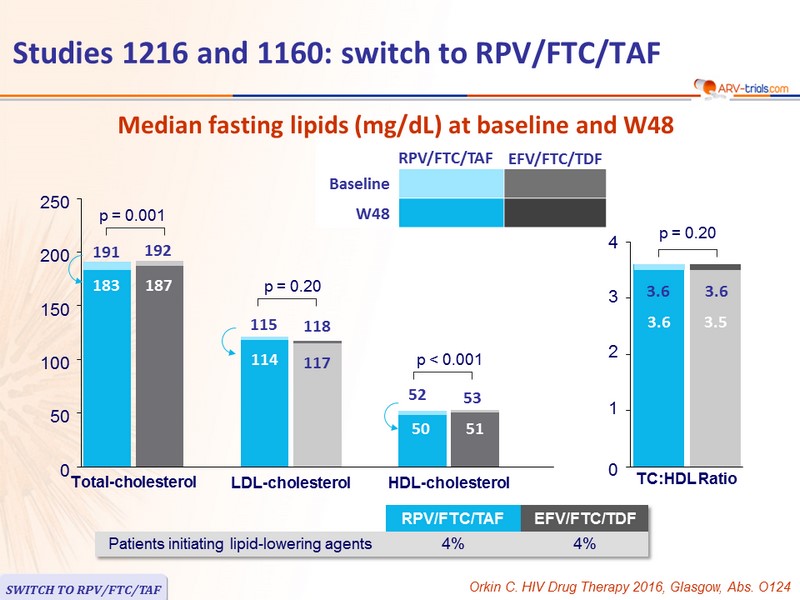
Median fasting lipids (mg/dL) at baseline and W48
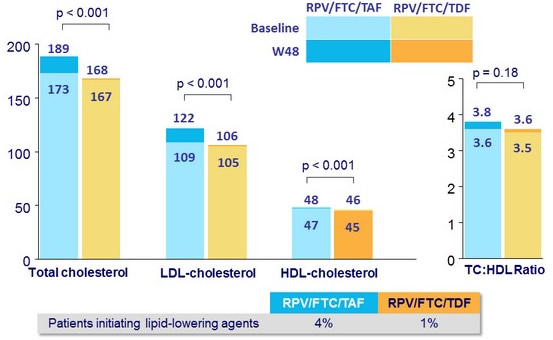
Median fasting lipids (mg/dL) at baseline and W48