Switch studies in virologically suppressed patients
Switch to DRV/r monotherapy
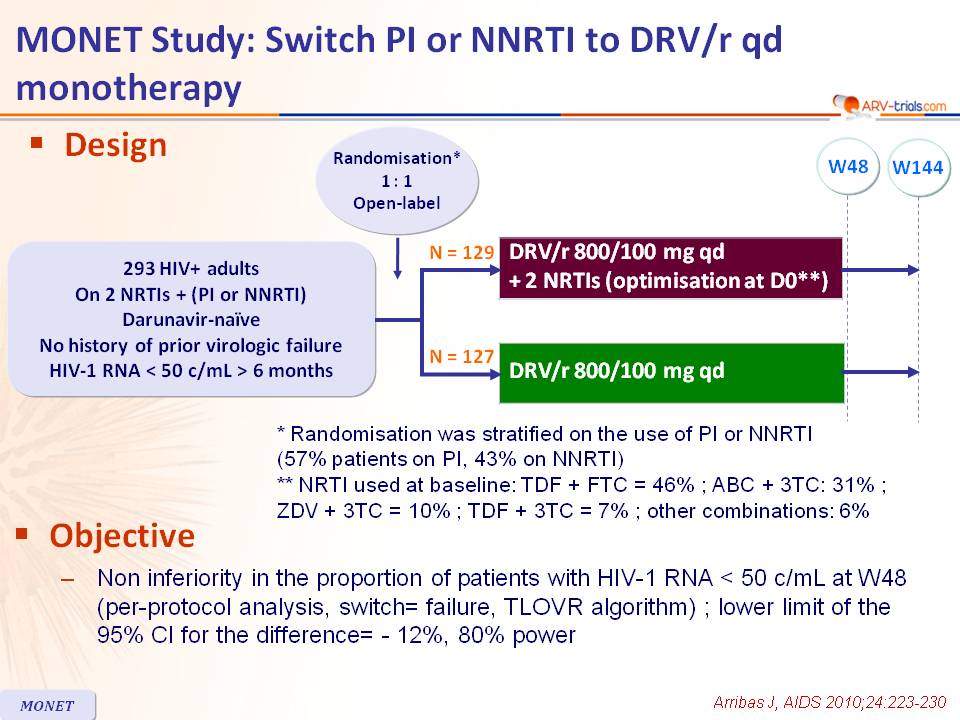
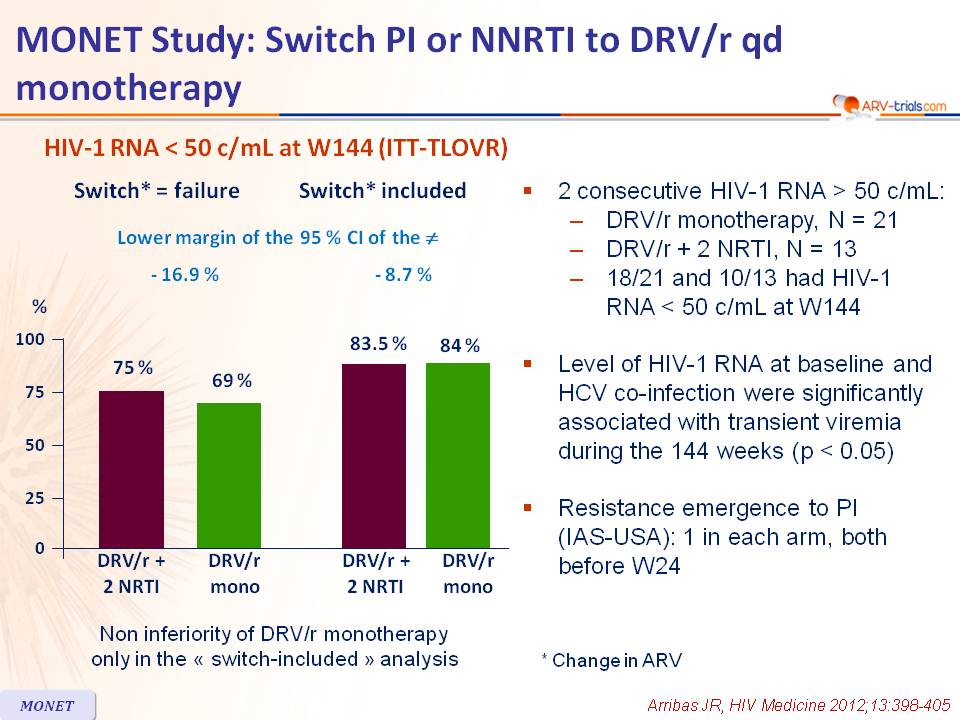
MONET Study: Switch PI or NNRTI to DRV/r qd monotherapy
Original article : AIDS. 2010 Jan 16;24(2):223-30 – JR Arribas ;
Rieger A, et al. AIDS 2010; Abs. THLBB209 ; HIV Med. 2012 Aug;13(7):398-405 – JR Arribas
Dernière mise à jour :
28/03/2014
Last update :
28/03/2014
Dr Anton Pozniak
Chelsea and Westminster Hospital
London, UK

- From W48 data
- In patients with virologic suppression on standard triple therapy (2 NRTIs + 1 NNRTI or 1 PI), once-daily DRV/r monotherapy has shown non inferior HIV RNA suppression at week 48 compared with a standard therapy of 2 NRTIs + once-daily DRV/r
- A switch to once-daily DRV/r monotherapy can be considered in patients who have HIV RNA < 50 c/mL for more than 6 months on other treatments and no history of virologic failure, but wish to avoid toxicities related to other ARVs

Design :
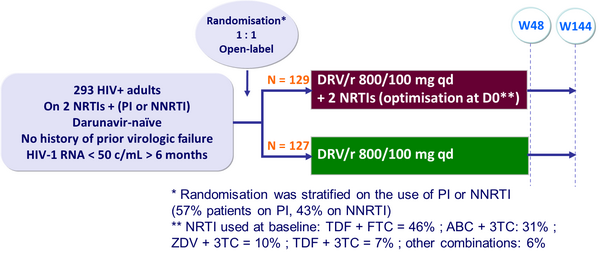
Objective :
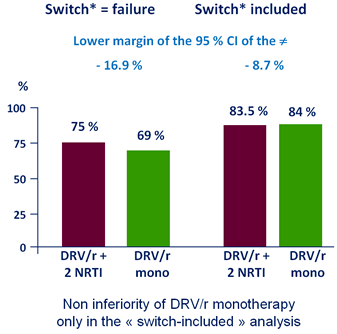
- Non inferiority in the proportion of patients with HIV-1 RNA < 50 c/mL at W48 (per-protocol analysis, switch= failure, TLOVR algorithm) ; lower limit of the 95% CI for the difference= - 12%, 80% power
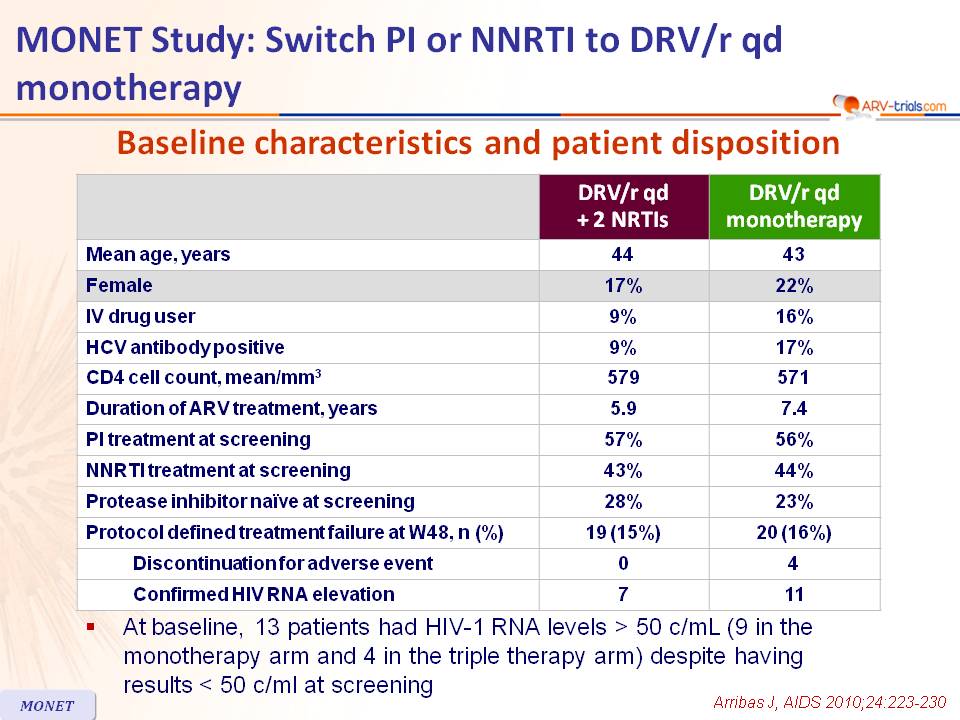
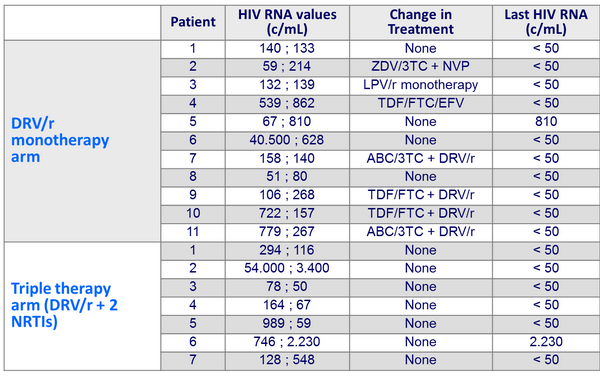
Baseline characteristics and patient disposition :
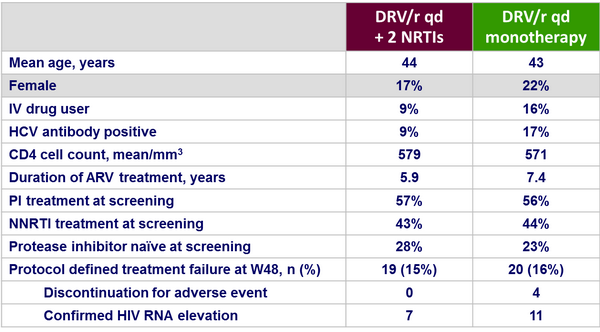
- At baseline, 13 patients had HIV-1 RNA levels > 50 c/mL (9 in the monotherapy arm and 4 in the triple therapy arm) despite having �results < 50 c/ml at screening
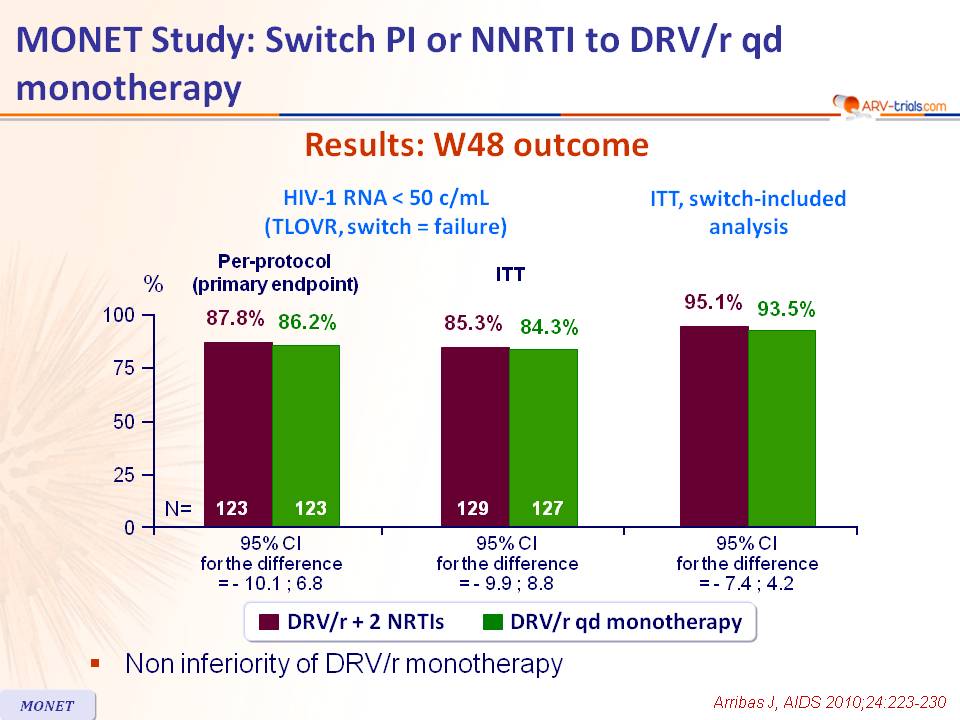
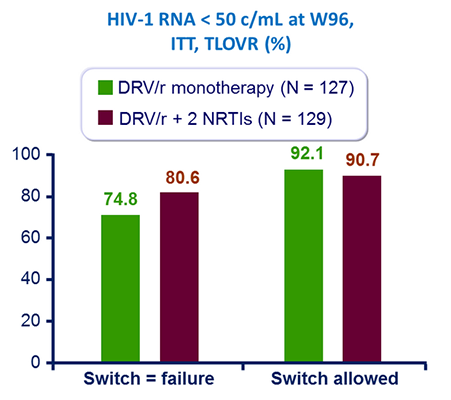
Results: W48 outcome :
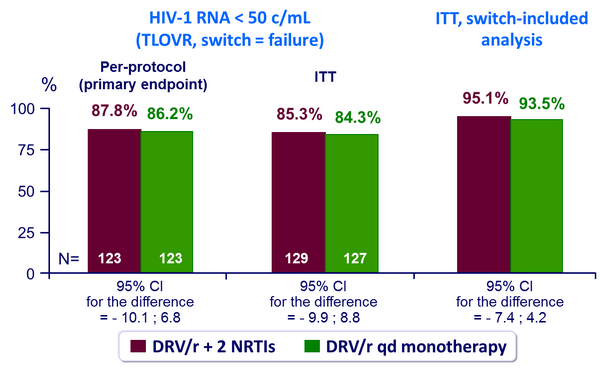
- Non inferiority of DRV/r monotherapy
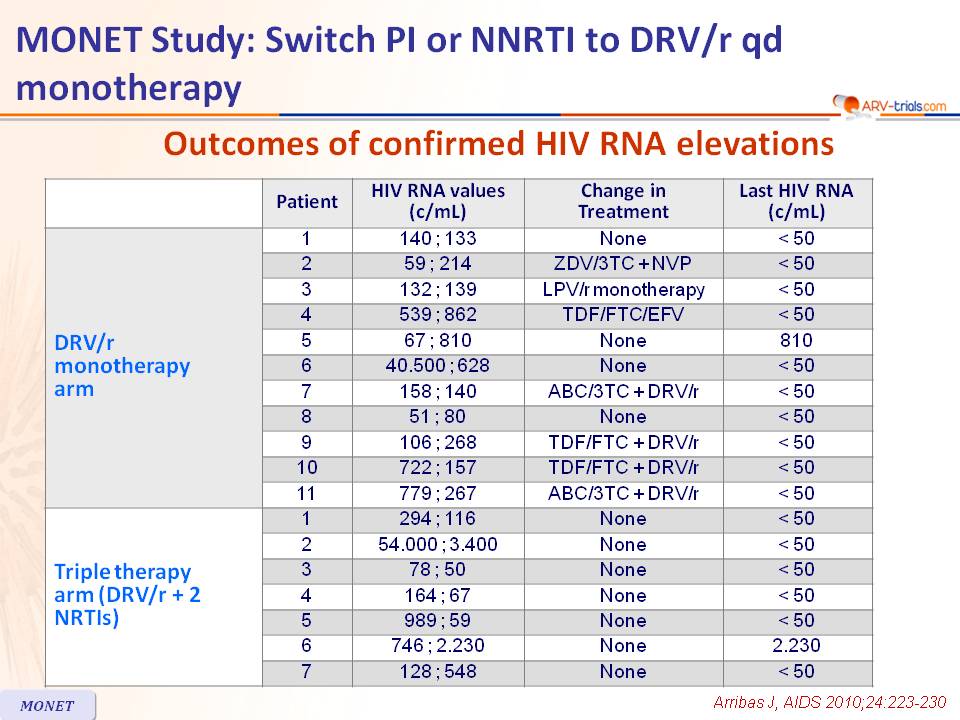
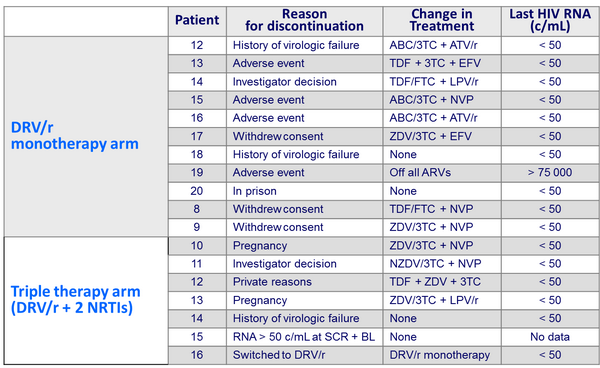
Outcomes of confirmed HIV RNA elevations :
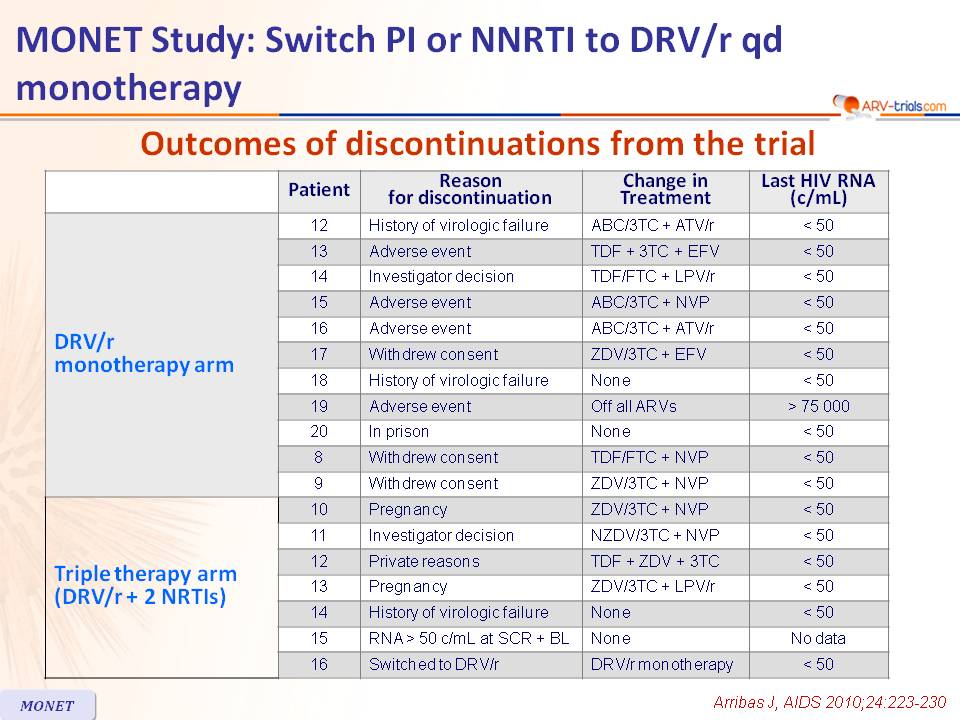
Outcomes of discontinuations from the trial :
Other endpoints :
- In multivariate analysis, hepatitis C co-infection was a significant predictor of confirmed HIV RNA elevations (p < 0.01)
- Resistance data: Genotype was available for 35/61 patients with HIV RNA > 50 c/mL (22 in the monotherapy group and 13 in the triple therapy group)
- Resistance mutations to PI in 1 one patient in each arm, with no phenotypic resistance to DRV. HIV-1 RNA returned to < 50 c/mL without changing therapy in both patients
- Most common grade 2 to 4 adverse events (AE) were gastrointestinal
- Serious AE were seen in 9 patients in each group
- Discontinuation for AE by W48 occurred in 8 patients in the monotherapy group and 3 in the triple therapy group
- Grade 1 to 4 nervous system AE were seen in 16% of patients in each group, and Grade 1 to 4 psychiatric AE in 9% of patients in each group
- There were more haematological abnormalities in the triple therapy arm,�related to zidovudine
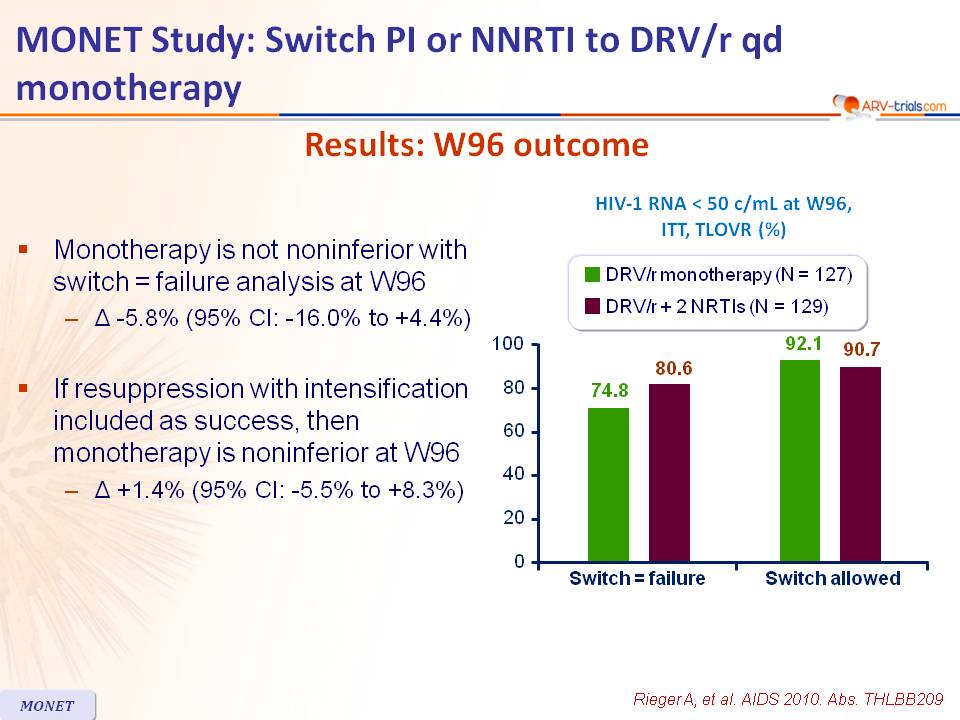
Results: W96 outcome :
- Monotherapy is not noninferior with switch = failure analysis at W96
- Δ -5.8% (95% CI: -16.0% to +4.4%)
- If resuppression with intensification included as success, then monotherapy is noninferior at W96
- Δ +1.4% (95% CI: -5.5% to +8.3%)
HIV-1 RNA < 50 c/mL at W144 (ITT-TLOVR) :
* Change in ARV
- 2 consecutive HIV-1 RNA > 50 c/mL:
- DRV/r monotherapy, N = 21
- DRV/r + 2 NRTI, N = 13
- 18/21 and 10/13 had HIV-1 RNA < 50 c/mL at W144�
- Level of HIV-1 RNA at baseline and HCV co-infection were significantly associated with transient viremia during the 144 weeks (p < 0.05)�
- Resistance emergence to PI �(IAS-USA): 1 in each arm, both before W24
 Back to Table of Contents Back to Table of Contents
|